Ovulation induction with follicular study
Ovulation induction is the process by which ovarian follicular development is stimulated by medications. This process is commonly practised and believed to induce follicular recruitment for those patients who are not ovulating (anovulation) or ovulating infrequently (oligo-ovulation). The most common clinical situation resulting in these ovulation defects is Polycystic Ovarian Disease (PCOD). Currently ovulation inducing drugs are used even in normally ovulating women and unexplained infertility cases with different protocols to increase the chances of pregnancy.
Depending on the purpose of ovulation inducing medications different processes are called
- Ovulation induction To induce recruitment of follicles in females with anovulation or oligoovulation.
- Ovulation augmentation/acceleration Trying to stimulate follicular response in normally ovulating females to increase the chances of pregnancy.
- Ovarian stimulation/Controlled ovarian hyperstimulation Mostly in IVF (In-vitro Fertilization) stimulation by injectable medication to gain multifollicular response
- Ovulation triggering To facilitate egg release/maturation from the follicle(s) by injectable medication. This will be helpful in females having anovulation or to time the egg release in IUI (Intra-uterine Insemination) or to attain egg maturation and to time egg pickup in IVF procedures
Ovulation induction with follicular study and scheduled intercourse is most commonly practised treatment for infertility. It is best suited for
- Women with < 30 years
- Short-term infertility ( <2 years of active married life)
- Where semen analysis is normal.
Pregnancy rates expected: 8-10% (8-10 couples out of 100 who get treatment with ovulation induction will get pregnancy in a month).
Procedures for scheduled intercourse
Natural cycle monitoring
- When menstrual cycle is regular
- No need for any medications
- Ultrasound monitoring only if needed to pinpoint ovulation timing or as and when required/advised by gynecologist. Trans-vaginal sonography is preferable for its accuracy.
- Sexual intercourse should be scheduled/advised around egg release time.
Natural cycle with ovulation trigger
- When ovulation induction is not needed.
- Ultrasound is necessary.
- Ovulation is triggered with injectable hCG hormone when the follicle(s) >18 mm with good triple line endometrial lining of >7 mm.
Cycle with ovulation induction
- When menstrual cycles are irregular or in some case with normal cycle as well
- Medication for ovulation induction is needed.
- Serial ultrasound is needed to monitor follicular growth.
- Intercourse is advised when the follicle(s) >18 mm with good triple line endometrial lining of >7 mm.
- Ovulation is either monitored using ultrasound or a trigger is given to plan ovulation timing and hence intercourse.
Ovulation inducing medication
- Oral medications: Letrozole or Clomiphene citrate - most commonly used. Wide range of doses and protocols are available. Commonly used protocol for Letrozole is 2.5-5 mg/day and for Clomiphene citrate is 50-150 mg/day, for 5 days starting between day 2 and day 5 of the cycle.
- Injectable medications: Gonadotropins are reserved for those cases where oral treatments are resistant. Various protocols but commonly used in the dose of 50-100 IU/day or alternate day till the follicle reaches >18 mm with good triple line endometrial lining of >7 mm.
Ovulation triggering medicines
- When the follicle reaches >18 mm with a good triple line endometrial lining of >7 mm, Ovulation can be triggered by following injectables.
- Human chorionic Gonadotropins (hCG): 5000IU/ 10,000IU of urinary highly purified hCG Intramuscular or 6500IU (250 mcg) recombinant hCG subcutaneously.
- GnRH agonist: 0.2 mg triptorelin or 0.5 mg of leuprorelin subcutaneously. Mostly in patients with the risk of OHSS. However, absence of leutrotopic action leads to premature leutiolysis and lower implantation (low pregnancy chances).
Ovulation should not be triggered with hCG if >3 follicles of >16 mm to avoid a complication called OHSS (Ovarian hyperstimulation syndrome).
Ovulation occurs 36 hours after the trigger to plan other procedures like IUI (Intra-Uterine Insemination) or intercourse accordingly.
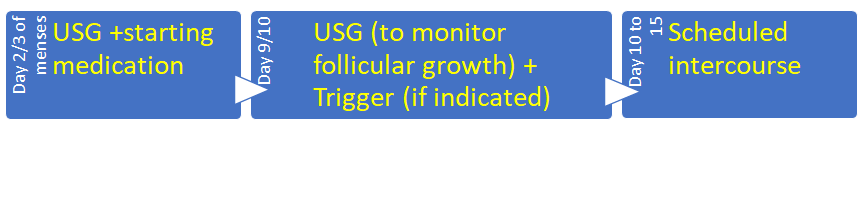
Timeline for this treatment